

The FDA already approved Cabenuva in January as the first complete HIV drug therapy to be taken once a month, but soon, Cabenuva may also be taken just once every two months.
The company that makes Cabenuva, ViiV Healthcare, has asked the Food and Drug Administration (FDA) to allow its long-acting injectable treatment to be taken every eight weeks instead of every four.
“Today’s submission of Cabenuva dosed every two months marks another meaningful step forward in our ongoing commitment to bring innovative HIV treatments to the community,” said Kimberly Smith, MD, MPH, Head of Research & Development for ViiV, in a press release dated February 24. (See “At the nexus of body and soul,” November + December 2020.) “This first-of-its-kind regimen reflects the evolving needs of people living with HIV, and, if this expanded use is approved, could allow adults living with HIV to maintain virologic suppression with six dosing days per year.”
Cabenuva is administered as two intramuscular long-acting injections, in the butt muscle. One injection consists of ViiV’s cabotegravir and the other of rilpivirine, from Janssen Pharmaceuticals. Injections begin after one month of taking oral forms of the medications (Vocabria and Edurant).
ViiV’s supplemental New Drug Application (sNDA) was submitted based on the results of a study showing that the two injections given once every eight weeks was non-inferior to administering them every four weeks. Those results came from the Phase 3b international clinical trial ATLAS 2-M (Antiretroviral Therapy as Long-Acting Suppression every 2 Months).
Before taking Cabenuva, individuals switching to it must already be on a stable anti-HIV regimen and have undetectable viral load (less than 50 copies), and have no history of antiviral drug failure or resistance to cabotegravir or rilpivirine.
For more about Cabenuva, go to Cabenuva.com or positivelyaware.com/Cabenuva.
DHHS recommendation on Cabenuva
An expert panel of the Department of Health and Human Services (DHHS) issued a recommendation in February that switching to Cabenuva to optimize treatment is seen as a good strategy.
“Based on the clinical trial results from two large randomized controlled trials [RCT, representing the gold standard in clinical research], the Panel recommends that once-monthly cabotegravir and rilpivirine intramuscular (IM) injections can be used as an optimization strategy for people with HIV currently on oral antiretroviral therapy (ART) with documented viral suppression for at least 3 months (although optimal duration is not defined) (A1 [recommendation]), who—
- Have no baseline resistance to either medication,
- Have no prior virologic failures [detectable viral load on treatment],
- Do not have active hepatitis B virus (HBV) infection (unless also receiving an oral HBV active regimen),
- Are not pregnant and are not planning on becoming pregnant [due to lack of data in this population],
- Are not receiving medications with significant drug interactions with cabotegravir and rilpivirine.”
“Before initiation of the IM injection, patients should receive oral cabotegravir and oral rilpivirine for 28 days as an oral lead-in period to assess tolerance to these drugs. Clinicians should refer to the product label for information regarding IM dose administrations as well as management strategies for planned or unplanned missed doses.”
Read more on the recommendation regarding Cabenuva at hivinfo.nih.gov.
The panel noted that, “Switching to long-acting injectable therapy can be advantageous in patients for a variety of reasons, including but not limited to reducing pill fatigue, disclosure concerns or stigma associated with taking daily oral medications, and to improve quality of life.”
Pediatric guidelines updated
A DHHS expert panel also updated its pediatric HIV guidelines. Several medications now have a different recommendation, based on new data. There’s also information added about telehealth communication and telemedicine vs. in-person clinic visits.
Per the update:
- With the release of a new, dispersible tablet formulation of dolutegravir (DTG) [Tivicay], DTG plus two new nucleoside reverse transcriptase inhibitors (NRTIs) is now recommended as a Preferred antiretroviral (ARV) regimen for infants and young children (aged 4 weeks and older and weighing 3 or more kg [6.6 pounds or more]) rather than being limited to children aged 3 and older and weighing 25 kg or more.
- Bictegravir (BIC), which is available as a component of the fixed-dose combination (FDC) tablet bictegravir/emtricitabine/tenofovir alafenamide (Biktarvy), is now recommended as a Preferred ARV regimen for children aged 6 years and older and weighing 25 kg and more [55 pounds and more].
- The Panel now recommends raltegravir (RAL) [Isentress] plus 2 NRTIs as an Alternative integrase strand transfer inhibitor-based regimen for children aged 4 weeks and older, rather than Preferred, because of its twice-daily dosing requirement and lower barrier to resistance compared to DTG or BIC.
- Although the FDA has approved abacavir (ABC) [Ziagen] in infants aged 3 months and older, based on reassuring safety data, the Panel recommends ABC plus lamivudine or emtricitabine as a Preferred dual NRTI backbone for use in infants and children aged one or more months old.
- With the ability to use ABC in infants and young children, zidovudine (ZDV) is now recommended as an Alternative NRTI for use in infants and children aged at least one or more months old.
Long-acting regimen in development: islatravir, lenacapavir
Another complete long-acting HIV regimen is in the works, and is being studied as both oral and injectable therapies.
Gilead Sciences and Merck announced an agreement to develop two of their long-acting drugs, still in clinical trials in combination with each other.
According to a joint press release in March, “Islatravir and lenacapavir are both potentially first-in-class medicines in late-stage clinical trials, with significant clinical data generated to date. Both medicines have long half-lives and have demonstrated activity at low dosages in clinical studies, which support development as an investigational combination regimen with long-acting formulations, both oral and injectable.”
The companies noted that, “While daily, single-tablet regimens are available for people living with HIV, options that would allow for less frequent, oral dosing or infrequent injections rather than daily dosing has the potential to address preference considerations, as well as issues associated with adherence and privacy.”
Merck is also developing islatravir in combination with the company’s doravirine (Pifeltro), and with doravirine and ViiV Healthcare’s 3TC (Epivir). Merck is also studying islatravir as a medication for PrEP (pre-exposure prophylaxis—prevention), including a once-monthly oral formulation.
Gilead’s lenacapavir has data supporting use as a subcutaneous injection administered once every six months, for both treatment of HIV and for prevention of the virus. Two PrEP studies are expected to begin this year.
The two medications come from drug classes not currently on the market. Merck’s islatravir is a nucleoside reverse transcriptase translocation inhibitor (NRTTI). Gilead’s lenacapavir is a capsid inhibitor. Clinical study of the combination is expected to start later this year.
Exciting news. Stay tuned.
PleasePrEPMe moves to HealthHIV
PleasePrEPMe.org, a comprehensive online educational resource originally created to bring together providers in California with people interested in PrEP (pre-exposure prophylaxis, or prevention) and PEP (post-exposure prophylaxis), has gone national and moved to HealthHIV.org. The user-friendly site provides information in both Spanish and English.
At the time PleasePrEPMe was formed in 2015, people interested in HIV prevention medications often had difficulty finding a receptive medical provider. This was true even with the emergency PEP schedule—treatment must be started within 72 hours of a known or suspected exposure to HIV.
“The opportunity to have been a part of creating a trusted, inclusive, welcoming source of HIV prevention information has been my honor,” said PleasePrEPMe founder Shannon Weber, a Renaissance woman who’s a social worker specializing in HIV services, an author, an advocate, and an artist. “I am confident HealthHIV will steward PleasePrEPMe to adapt and change in response to community needs.”
HealthHIV provides an extensive number of HIV prevention and care training and education programs, for both individuals and health care workers.
Out of the Closet thrift store opens in Orlando
Los Angeles-based AIDS Healthcare Foundation (AHF) has opened another of its Out of the Closet thrift stores, in Orlando, Florida. As with its other thrift shops around the country, the store will house a pharmacy and offer free rapid tests for HIV and a number of STIs.
“The grand opening [in February offered] the chance for Orlando shoppers to be among the first to discover the unique finds and hidden treasures for which ‘Out of the Closet’ is famous,” said Jonathan Kreuyer, general manager of the stores, in an AHF press release. “With 23 other locations in California, Florida, Ohio, Georgia, and New York, AHF’s Out of the Closet Thrift Store chain is the nation’s largest retail fundraising venture for HIV/AIDS services, and 96 cents of every dollar earned is directed towards local HIV/AIDS awareness efforts and AIDS care to those in need.”
Unlike the past, AHF now believes in PrEP.
Housing Works offers thrifting online
Housing Works opened an online version of its own thrift stores back on National Thrift Store Day, August 17. This version specializes in high-end designer and vintage goods. The selection is small, but exquisite. Sometimes funky fun. And not necessarily a piggy-bank-breaker.
The New York-based non-profit, in existence for more than 30 years, provides housing and support services for homeless and unstably housed people living with HIV. It operates 10 thrift stores dotting Manhattan and Brooklyn. Go to eshop.housingworks.org.
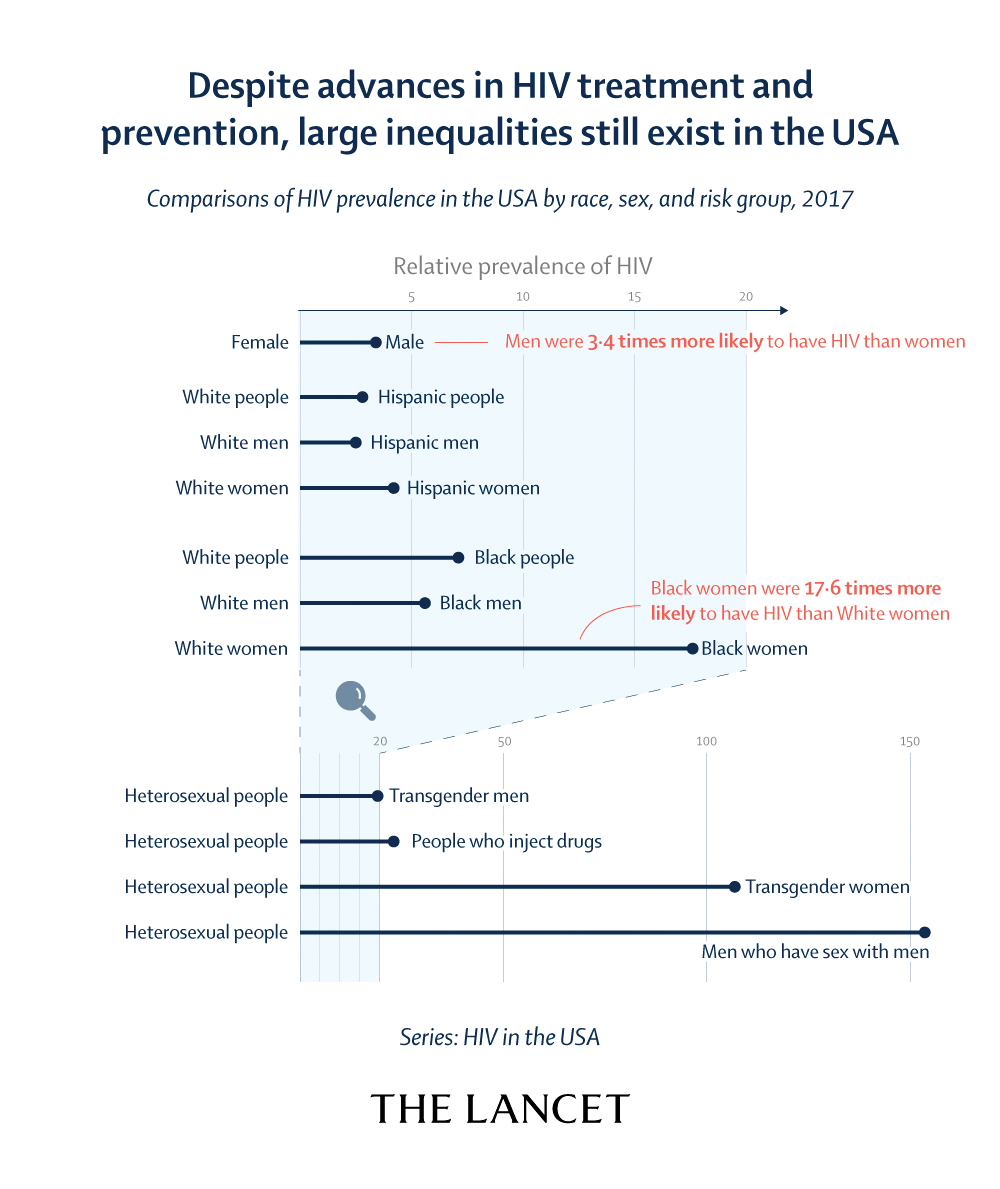
Lancet’s call to action on Ending the HIV Epidemic
The Lancet Series “HIV in the USA” from the February 19 issue concludes with a “Call to Action” outlining the measures needed for Ending the HIV Epidemic initiative to succeed. Among the many items addressed in the call to action, U=U (Undetectable Equals Untransmissable, an education campaign about how undetectable HIV virus may pose no threat of transmission) has a critical role to play. Ensuring that people living with HIV have the treatment and services they need to achieve and maintain an undetectable viral load not only saves lives, but also prevents new transmissions.
The Call to Action states:
- A national culturally competent effort is needed to raise awareness of U=U as a promising approach to reduce HIV stigma, which has a powerful potentiating role in both acquisition risks and treatment challenges.
- Health-care professionals need to inform patients living with and affected by HIV about U=U to improve, first and foremost, personal health, as well as public health; sharing this information might greatly improve the social and emotional wellbeing of people living with HIV, reduce HIV stigma, reduce anxiety associated with HIV testing, and help motivate treatment uptake, treatment adherence, and engagement in care.
- Advocates should be equipped to use the so-called public health argument from U=U in advocacy to increase access and remove barriers to quality health care; ensuring people with HIV have the treatment and services they need to achieve and maintain an undetectable viral load not only saves lives, but also is an effective way to prevent new transmissions.
- Providers should advocate for use of the concept of Undetectable equals Untransmittable (U=U) in messaging and support all patients to remain virally suppressed.
- To view the entire series, go to thelancet.com/series/HIVinUSA.
—Michael Broder

DHHS updates HIV and COVID-19 recommendations
The Department of Health and Human Services (DHHS) on February 26 updated its COVID-19 recommendations for people living with HIV (PLWH). Of note: PLWH should get vaccinated; it’s still not known if HIV leads to a greater risk for COVID-19 infection. Much of the new information is provided below. There is also a discussion of COVID-19 treatments, which should be used the same way in people living with HIV as in the general population. Read the updates at clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/HIV_COVID_19_GL__2021.pdf.
HIV and COVID-19
According to the update, “Whether people with HIV are at greater risk of acquiring SARS-CoV-2 infection is currently unknown. Data on the clinical course of COVID-19 in people with HIV are emerging. In the initial case series from Europe and the United States, no significant differences in clinical outcomes were found between people with HIV who developed COVID-19 and individuals without HIV. For example, data from the Veterans Aging Cohort Study compared outcomes in 253 mostly male participants with HIV and COVID-19 who were matched with 504 participants with only COVID-19. In this comparison, no difference emerged in COVID-19 related hospitalization, intensive care unit (ICU) admission, intubation, or death between patients with or without HIV. In contrast, worse outcomes, including increased COVID-19 mortality rates, in people with HIV have been reported in other cohort studies from the United States, the United Kingdom, and South Africa. In a multicenter cohort study of 286 patients with HIV and COVID-19 in the United States, lower CD4 count (less than 200 cells/mm), despite virologic suppression [undetectable viral load], was associated with a higher risk for the composite endpoint of ICU admission, mechanical ventilation, or death. In another study of 175 patients with HIV and COVID-19, a low CD4 count or CD4 nadir [lowest number ever found] was associated with poor outcomes. In a cohort study in New York, people with HIV had higher rates of hospitalization and mortality with COVID-19 compared to people without HIV.
“In the general population, individuals who are at highest risk of severe COVID-19 include those older than 60; those who are pregnant; and those with comorbidities, such as obesity, diabetes mellitus, cardiovascular disease, pulmonary disease, smoking history, sickle cell disease—as well as solid organ transplant recipients,” the report continued. “Many people with HIV have one or more comorbidities that may put them at increased risk for a more severe course of COVID-19. Both COVID-19 and HIV disproportionately affect communities of color. Based on the available literature, close monitoring is warranted for all people with HIV and SARS-CoV-2 infection, especially those with advanced HIV or with comorbidities.”
Vaccination in HIV
“People with HIV should receive SARS-CoV-2 vaccines, regardless of CD4 or viral load, because the potential benefits outweigh potential risks,” the guidelines advise.
- “Based on recent literature to date, people with HIV appear to be at increased risk for severe outcomes with COVID-19 compared with people without HIV and should be included in the category of high-risk medical conditions when developing vaccine priority.
- “People with HIV were included in clinical trials of the two mRNA vaccines; at this time, the safety and efficacy in this specific subgroup have not been fully reported. People with HIV who are well controlled on antiretroviral therapy (ART) typically respond well to licensed vaccines. Guidance for these vaccines, including for people with HIV, is available through the Advisory Committee on Immunization Practices (ACIP) and from the Infectious Diseases Society of America (IDSA). Confidentiality about their underlying condition should be preserved when administering vaccines to people with HIV.
- “Current recommendations of the ACIP, the American College of Obstetricians and Gynecologists (ACOG), and the Society of Maternal Fetal Medicine (SMFM) state that pregnant and lactating people who otherwise meet criteria for vaccination should not be restricted from vaccine access (ACOG, 2020). The CDC also provides information about vaccine considerations for people who are pregnant and breastfeeding.”
Links are provided in the document.
Other new considerations
“New onset or worsening dyspnea [difficulty breathing] warrants in-person evaluation.”
“Patients and/or caregivers should be aware of warning signs and symptoms that warrant in-person evaluation, such as new dyspnea, chest pain/tightness, confusion, or other mental status changes.”
“Be aware that people with HIV with additional comorbidities may be eligible for one of the anti-SARS-CoV-2 monoclonal antibodies available through Emergency Use Authorization from the FDA.”
Added to the paragraph on greater risks of domestic violence during quarantine are the italicized words here, “Reports indicate that some measures designed to control the spread of COVID-19 may increase the risk of intimate partner violence and/or child abuse, as well as limit the ability of people to distance themselves from abusers or to access external support. Providers should assess patient safety at each clinical encounter, either in-person or via telemedicine, being cognizant of the patient’s ability to speak privately.”
Clinicians are referred to the NIH COVID-19 Treatment Guidelines (covid19treatmentguidelines.nih.gov/whats-new), which have a section on “Special Considerations in People with HIV.”
A lengthy section on pregnancy and another on children living with HIV have been added.