
Nearly four decades of HIV activism in the United States has demonstrated a movement with strong foundations in fighting for access to lifesaving prevention and treatment. Unfortunately, these efforts have not equitably benefited communities disproportionately impacted by HIV, in particular, Black people. We bear the brunt of the HIV burden, experience the worst care outcomes across the HIV care continuum and are characterized as lower utilizers of biomedical HIV prevention technologies including oral PrEP. So, let us heed the wise words of the late U.S. Representative John Lewis and build a movement for Black people by Black people to fight for what we deserve.
Recently, the U.S Food and Drug Administration (FDA) approved the first non-oral, long-acting injectable treatment (cabotegravir and rilpivirine, brand name Cabenuva). A long-acting injectable prevention option (cabotegravir, brand name Apretude) resulting from findings of key research studies led by the HIV Prevention Trials Network (NPTN 083 and 084) promises to reconsider paradigms of pill burden and challenges to medication adherence among groups who are undoubtedly overrepresented among incident and prevalent HIV diagnoses.
In a press release about the new drug approvals, the FDA declared that long-acting formulations offer “a tremendous opportunity to narrow racial disparities in HIV incidence.”
As folks who advocate with Black-focused social justice and health equity-oriented lenses, we offer that statements like these overstate the perceived benefits of long-acting prevention and treatment. They oversimplify complex historical systems of exclusion that limit equity in access to HIV treatment and prevention advances and threaten to perpetuate narratives that medicalize adherence while ignoring social contexts that facilitate negative health outcomes among Black people.
As long-acting options enter the HIV treatment and prevention landscape, we are challenged by the current state of affairs of HIV treatment and prevention among Black people. For example, more than 10 years after the approval of the first oral biomedical HIV prevention strategy in the U.S., data from the CDC says that only 11% of Black people with an indication for PrEP have actually been prescribed it. Indeed, Black communities may not have felt the the “game changing” benefits of oral PrEP once promised by the field. What we experience instead are provider biases, barriers to medication coverage by insurers and high lab costs, to name a few. It remains to be seen whether or not Black communities will benefit from the benefits of long-acting injectables. As of the time this article was written, we were unable to locate any online data sources that provided any demographic data on long-acting injectable users for prevention or treatment. This is abhorrent. For data on global PrEP, we recommend PrEPWatch, a global resource for PrEP information and resources.
To make good on the promises of long-acting HIV prevention and treatment, stakeholders working in HIV must support community-derived strategies for Black people led by and developed by Black people to support our collective improved health. As a matter of health justice, we demand the continued acknowledgement and remedying of historical social and structural factors that limit Black people’s sustained engagement in HIV care.
The history of exploitation, subjugation of and experimentation on the Black body must be addressed, or the cycle will continue. James Marion Sims’s (the “Father of Gynecology”) exploitation of the Black female body, the U.S. Public Health Service study “Untreated Syphilis in the Negro Male” at Tuskegee and the stolen cancer cells from Henrietta Lacks, which were used to advance modern science, are just a few examples of why there is a culture of distrust in research, medicine and new health technologies, including long-acting injectables.
The impact that anti-Black racism, discrimination, generational poverty and sexism has had in limiting our ability to equitably access HIV care is beyond calculation. As it relates to long-acting modalities, we can only predict the same negative impacts will limit Black people’s utilization. Specifically, anti-Black racism and discrimination, medical distrust and the fact that many providers do not treat Black patients the same as White counterparts continue to have a detrimental impact on the ability of Black people to access HIV prevention and treatment options.
PrEP in Black America Coalition
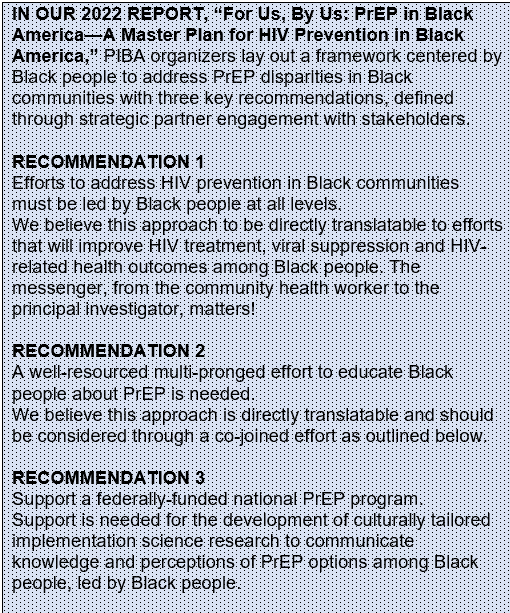
In the spirit of seeking change to ameliorate the devastating impact of HIV in Black communities through biomedical HIV prevention, Black leaders from across the nation established the PrEP in Black America (PIBA) Coalition in 2022. We offer as a remedy to these historical injustices reimagined interventions and strategies designed for Black people by Black people. Further, we advocate for interventions and strategies as described in Goal 3 of the National HIV/AIDS Strategy for the United States, 2022-2025, that “Reduce HIV-related disparities as health inequities” while increasing the recognition of racism as a public health crisis.
We acknowledge the work of PIBA as a model for effective community engagement and mobilization through an HIV prevention lens with features that are fully translatable to the HIV treatment space. Since its establishment, the PIBA coalition has organized two summits that brought together over 250 Black HIV prevention leaders and public health practitioners to discuss strategy, interventions and policy as it relates to access to HIV prevention tools in the Black community.
It is important that we learn from our experience with treatment and prevention inequities and apply them to the rollout and implementation of long-acting injectables. To get to the root of these inequities that affect the Black community, we must address medical mistrust of the health care system. This is a phenomenon that has been apparent throughout U.S. history stemming in large part from the medical mistreatment and abuse of Black people dating back to slavery.
Black people are not categorically challenged by medication adherence. The public narrative around PrEP and treatment adherence among Black people obscures root causes, like racism and medical mistrust, making these trends appear natural and inevitable. Our ability to effectively maintain adherence and secondarily viral suppression exists within a system that does not support our lived experience.
And to be clear, if we are to benefit from access to long-acting injectables, they must be accessible and affordable.
As public health practitioners and founding members of the PrEP in Black America Coalition, we engage with colleagues and allies to raise, nurture and articulate an effective social justice public narrative that supports a common agenda to achieve health and racial equity. Without a clear and concise consideration of the social and ecological contexts of Black people, we will continue to miss the proverbial boat and risk not benefiting from long-acting prevention and treatment modalities.
There is a social and moral obligation for systemic change.
If you see something that is not right, not fair, not just, you have a moral obligation to do something about it.
—U.S. Representative John Lewis
(1940—2020)
Black public health professionals, advocates, activists and organizers can subscribe to the PIBA listserv, tinyurl.com/pibalistserv. Follow @prepinblackamerica on Instagram and @PrEPInBlkUS on X (formerly Twitter).

Danielle M. Campbell, MPH, is a community advocate living in Los Angeles and a founding member of the PrEP in Black America Coalition.

John W. Meade, Jr., MPH, is senior policy program manager at AVAC, based in New York City, and a founding member of the PrEP in Black America Coalition.